procedural planning for Crown Thinning
Restoring natural vertex architecture through precise whorl design, strategic graft allocation, and integrated medical stabilization.
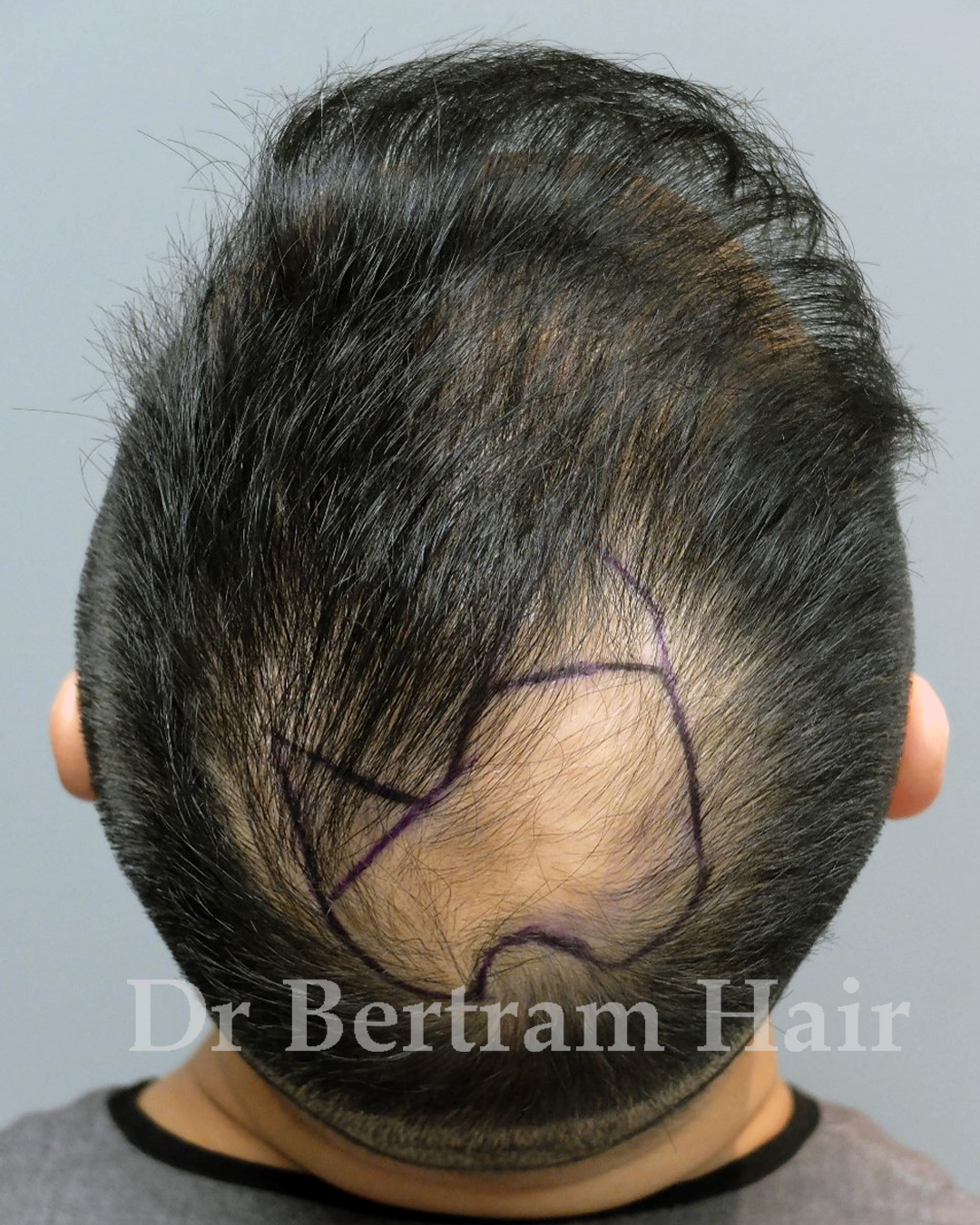
Before
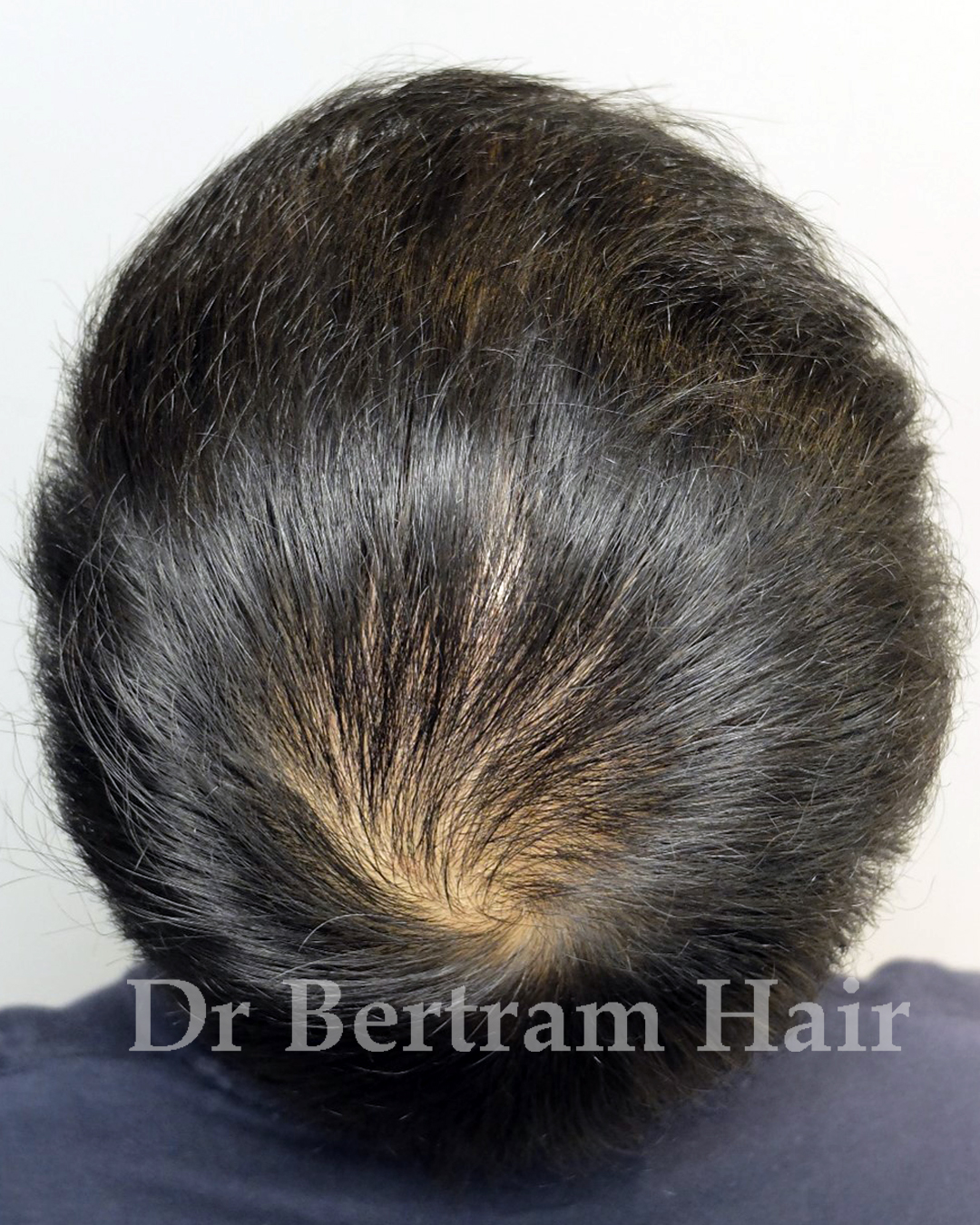
After Hair Transplant
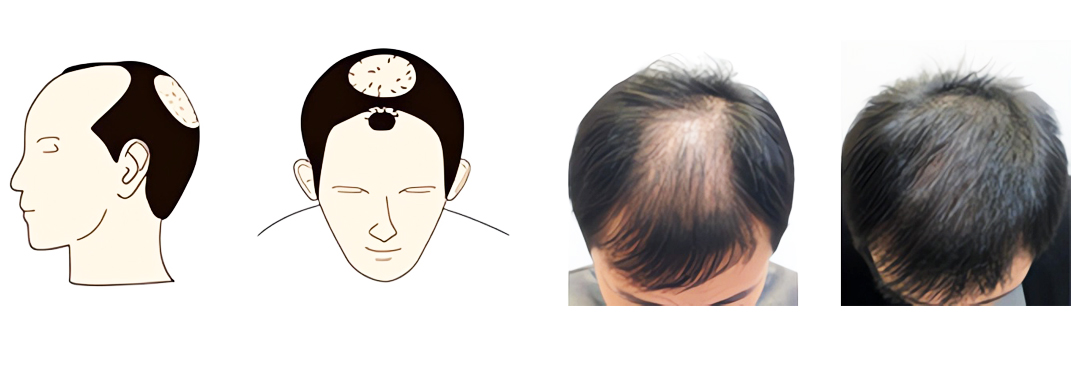
What Causes Thinning on the Top of the Scalp?
- Genetics & DHT: Vertex hair loss is driven by genetics and DHT — follicles in crown are genetically sensitive, leading to miniaturization.
- Health correlations: Some studies suggest correlation between early-onset vertex baldness and increased risk of coronary heart disease. Patients with rapid vertex loss may benefit from general health evaluation.
Who Is a Suitable Candidate?
✅ Ideal Candidate
- Stable defined bald spot
- Robust donor density (1,500–2,500+ grafts available)
- Realistic goals — improved coverage, not full adolescent density
- Commitment to medical therapy
❌ Poor Candidate
- Diffuse, unstable thinning (DUPA)
- Limited donor reserve
- Unrealistic expectations or refusal of medical therapy
- Young age (<25) with aggressive loss — stabilize medically first
Surgical Strategy & Long-Term Planning
💡 Whorl reconstruction
Incorrect angulation leads to unnatural appearance.
Incorrect angulation leads to unnatural appearance.
💡 Density strategy
30–40 FU/cm² — swirling pattern creates optical illusion of fullness.
30–40 FU/cm² — swirling pattern creates optical illusion of fullness.
💡 Graft estimates
Norwood III/IV: 1,200–1,800 grafts. Norwood V+: 2,000–2,500+ grafts.
Norwood III/IV: 1,200–1,800 grafts. Norwood V+: 2,000–2,500+ grafts.
💡 Front vs. Crown Priority
If donor limited, frontal framing takes priority — greater aesthetic impact than dense crown.
If donor limited, frontal framing takes priority — greater aesthetic impact than dense crown.
💡 Medical Therapy
Finasteride stabilizes native hair — prevents "halo" of thinning around restored crown.
Finasteride stabilizes native hair — prevents "halo" of thinning around restored crown.
💡 Future-Proofing
Account for future expansion of bald area. Over-committing grafts to crown early jeopardizes long-term pattern.
Account for future expansion of bald area. Over-committing grafts to crown early jeopardizes long-term pattern.
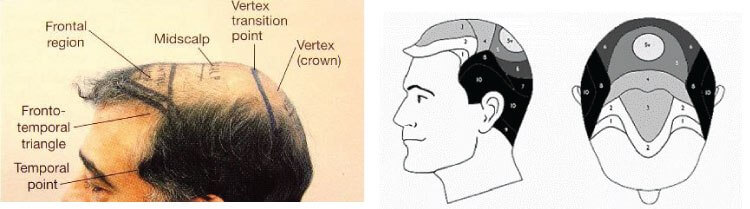
Strategy for Advanced Norwood (V–VII)


- Class V-VI: Create defined core of coverage in central crown. Second session for added density.
- Class VII: Limited donor — prioritize frontal frame or create central crown "oasis." Full coverage unrealistic.
Frequently Asked Questions
Q: Is crown transplant more difficult than hairline?Yes. Requires recreating complex whorl pattern. Incorrect angulation results in unnatural appearance.
Q: How many grafts for full crown coverage?Norwood III/IV: 1,200–1,800. Norwood V+: 2,000–2,500+. Multiple sessions may be needed.
Q: Will transplanted crown hair fall out?No. Transplanted hair is DHT-resistant and permanent. Native hair around it may continue to thin without medication.
Q: Do I need Finasteride after crown transplant?Strongly recommended. Without it, surrounding native hair may recede, creating an isolated "island" of transplanted hair.