What is Hair Transplant?
Clinical overview and scientific basis of Follicular Unit Excision.
Part 1: Scientific Basis of Hair Transplantation
Historical Development
Modern hair transplantation began in the 1950s when Dr. Norman Orentreich demonstrated that hair follicles transplanted from the back and sides of the scalp continued to grow in their new location. This observation, later formalised as the principle of donor dominance, established that hair follicles retain their genetic characteristics regardless of where they are transplanted. This principle remains the foundation of all hair restoration surgery today.
The procedure has since gained international recognition, with patients including public figures, former heads of state, and celebrities worldwide having undergone hair restoration. The field has evolved from the early 4mm "plug" grafts to modern micro-surgical techniques that produce natural, undetectable results.
Two Types of Hair
Human scalp hair can be categorised into two distinct types based on their response to hormonal influence:
- Androgen-sensitive hair: Found on the frontal scalp, crown, and vertex. These follicles contain androgen receptors and are susceptible to miniaturisation under the influence of dihydrotestosterone (DHT). This sensitivity is the underlying cause of androgenetic alopecia (pattern hair loss).
- Androgen-insensitive hair: Found in the occipital (back) and temporal (side) regions. These follicles lack significant androgen receptors and are genetically resistant to DHT. When transplanted to balding areas, they retain this resistance and continue to grow permanently — the principle of donor dominance.
Worldwide Trends in Hair Restoration

Hair transplantation has become one of the fastest-growing aesthetic procedures globally. According to the International Society of Hair Restoration Surgery (ISHRS), over 730,000 hair transplant procedures were performed worldwide in 2022. The procedure is now available in over 70 countries, with increasing demand driven by technological advancements, reduced recovery times, and growing social acceptance.
Part 2: The Hair Transplant Procedure
Hairline Design
The procedure begins with preoperative planning. The surgeon assesses the patient's facial proportions, age, and hair characteristics to design a hairline that is age-appropriate and naturally framed. Key considerations include the anterior hairline position, temporal recessions, and the transition zone between the hairline and the frontal scalp.
Graft Extraction
Grafts are harvested from the donor area using micro-punches (0.7–0.9mm). Each follicular unit — containing 1 to 4 hairs — is extracted individually. The number of grafts extracted depends on the patient's donor density, scalp laxity, and the extent of the recipient area.
Incision and Insertion
Recipient sites are created using micro-blades or needles, with the orientation, angle, and depth determined by the natural hair direction in the recipient area. Grafts are then inserted into these sites by the surgical team, with attention to density, distribution, and natural hair growth patterns.
Aftercare and Post-Operative Management
Post-procedure care includes specific instructions on wound care, sleeping position, and activity restrictions. Follow-up visits are scheduled to monitor graft survival, assess healing, and provide guidance on ongoing hair care.
Part 3: Modern Techniques in Hair Restoration
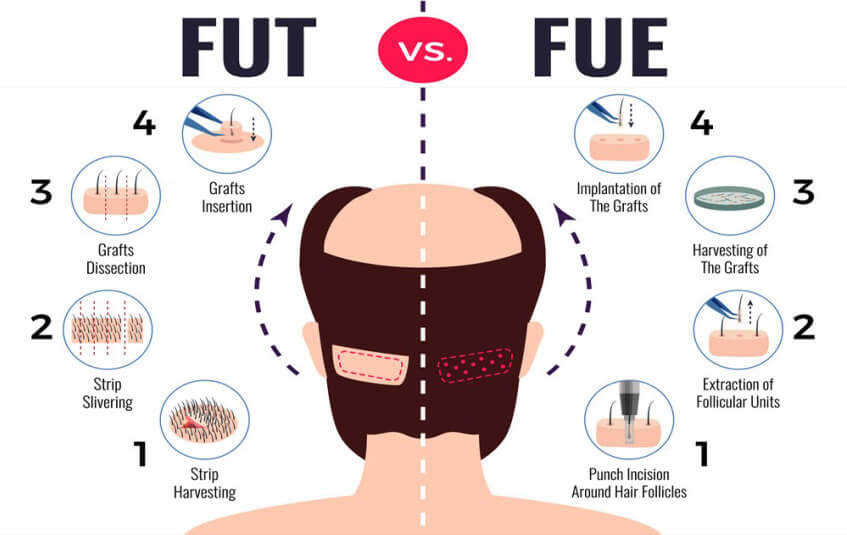
FUT / STRIP
Follicular Unit Transplantation (FUT) involves harvesting a strip of tissue from the donor area. The strip is then dissected into individual follicular units under magnification. This technique typically yields a higher number of grafts per session.
FUE
Follicular Unit Excision uses micro-punches to extract individual grafts directly from the donor area. This technique leaves no linear scar and is associated with faster recovery times.
Robotic
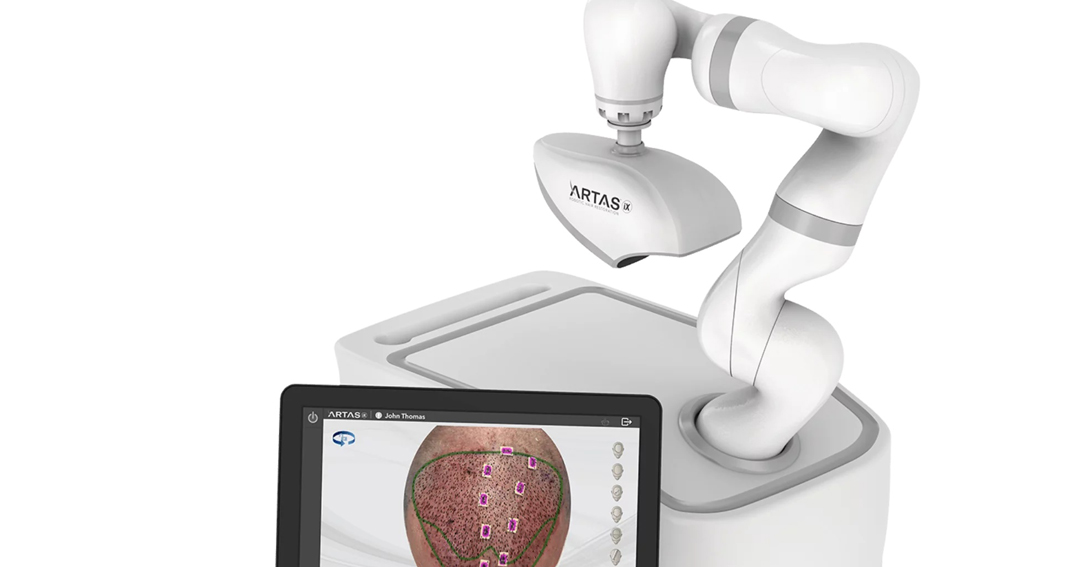
Robotic-assisted systems use imaging technology to identify and harvest grafts with automated precision. The system assists in graft selection and extraction, with the surgeon overseeing the process.
COMBO - FUE & FUT Combination
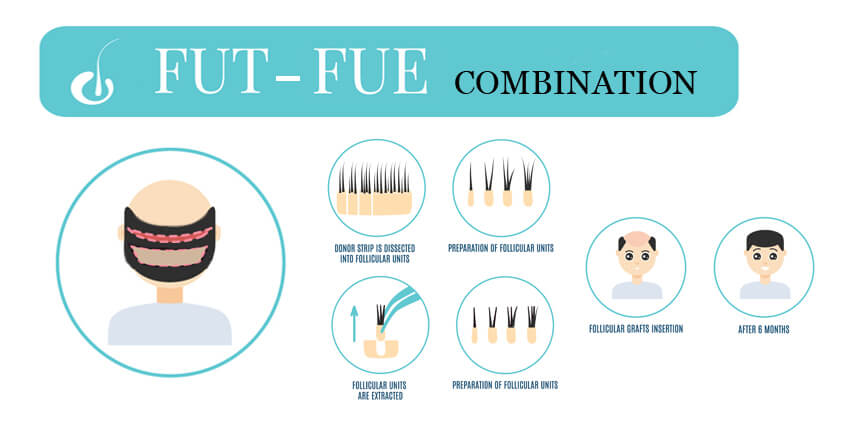
Some surgeons use a combined approach, utilising different techniques for different areas of the scalp. This may involve FUE for smaller sessions or specific areas, and FUT for larger sessions requiring a higher graft count.
Part 4 : Our Clinic's FUE Approach

Since 2024 our clinic exclusively uses the FUE (Follicular Unit Excision) technique. This approach is selected for its clinical advantages, including the absence of a linear scar, faster recovery times, and the ability to harvest grafts from a wider donor area. The technique is performed using motorised instrumentation combined with manual manoeuvring of the depth, angle, and speed of the 0.8mm extraction punch.
Our FUE Category : Full-Thickness Skin Graft
A full-thickness skin graft (FTSG) is a portion of skin completely detached from its original blood supply and transferred to a new location. It contains:
- Complete epidermis: The outermost layer from which hair shafts emerge.
- Full dermis: Contains sebaceous glands, arrector pili muscles, and follicular bulbs.
- Adnexal structures: Hair follicles, sebaceous glands, sweat glands, and associated stem cell niches.
An FUE graft harvested with a 0.8mm diameter punch contains the same anatomical components as the original 4mm "plug" grafts — only the scale differs. The classification of FUE as a full-thickness skin graft is consistent with clinical and regulatory definitions.
Intact Graft Transfer
A fundamental characteristic of our FUE is that the entire follicular unit is transferred unaltered (other than trimming excess fat for ease of insertion). It is therefore a complete, viable tissue unit — not a processed cellular suspension. This distinguishes FUE from procedures such as PRP (centrifuged blood) or regenerative cell therapy (processed tissue), where the original tissue structure is disrupted.
Our Safety Metrics — Total Body Surface Area (TBSA)
A 0.8mm diameter punch creates a circular defect with an approximate area of 0.005 cm² per graft. A 3,000-graft FUE session removes less than 0.1% of total body surface area. The following tables quantify the total tissue removed in FUE procedures.
Average Adult Male (1.9 m² = 19,000 cm²)
| Grafts | Total Area (cm²) | % of TBSA |
|---|---|---|
| 2,000 | ~10 cm² | ~0.053% |
| 3,000 | ~15 cm² | ~0.079% |
| 4,000 | ~20 cm² | ~0.105% |
| 5,000 | ~25 cm² | ~0.132% |
Average Adult Female (1.6 m² = 16,000 cm²)
| Grafts | Total Area (cm²) | % of TBSA |
|---|---|---|
| 2,000 | ~10 cm² | ~0.063% |
| 3,000 | ~15 cm² | ~0.094% |
| 4,000 | ~20 cm² | ~0.125% |
| 5,000 | ~25 cm² | ~0.156% |
Grafts Needed to Reach 1% TBSA
Adult male: ~38,000 grafts.
Adult female: ~32,000 grafts.
Typical lifetime donor supply is 4,000–8,000 grafts. Even the largest FUE sessions remove only a small fraction of the allowable limit.
Selected References
- Orentreich N. Autografts in alopecias and other selected dermatological conditions. Annals of the New York Academy of Sciences. 1959;83:463-479.
- Rassman WR, Bernstein RM, McClellan R, Jones R. Follicular unit extraction: minimally invasive surgery for hair transplantation. Dermatologic Surgery. 2002;28(8):720-728.
- Headington JT. Transverse microscopic anatomy of the human scalp. Archives of Dermatology. 1984;120(4):449-456.
- International Society of Hair Restoration Surgery. 2022 Practice Census Report. ISHRS; 2023.